If you or someone you love just heard the word “diabetes” from a doctor, your mind is probably racing. Type 1 or Type 2 does it even matter which one? It does, and the difference is bigger than most people realize.
Both conditions share a name and a core problem: blood sugar that climbs too high. But they start differently, progress differently, and are treated differently. Mixing them up can lead to the wrong assumptions about diet, weight, insulin, and even who’s “at fault” for the diagnosis (no one is).
This guide breaks down exactly how Type 1 and Type 2 diabetes differ and where they overlap so you can understand what’s happening in the body and what comes next.
Quick Answer: The Core Difference
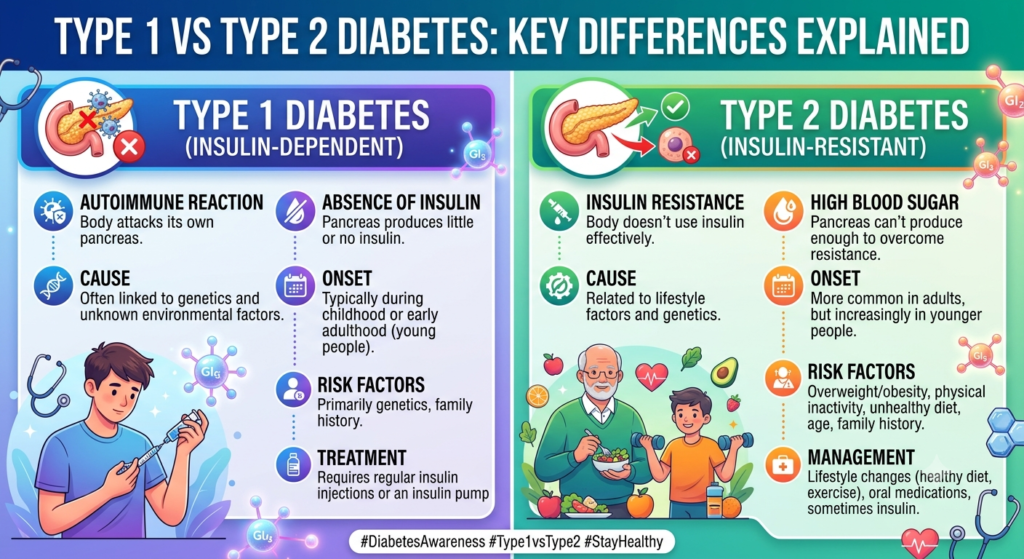
Type 1 diabetes is an autoimmune disease. The immune system destroys the insulin-producing cells in the pancreas, so the body makes little or no insulin at all. Type 2 diabetes is a metabolic condition. The pancreas still makes insulin, but the body’s cells stop responding to it properly a problem called insulin resistance. Over time, the pancreas can’t keep up, and blood sugar rises.
In short: Type 1 is about insulin production. Type 2 is about insulin resistance, which can eventually affect production too.
How Insulin Normally Works
To understand either condition, it helps to know what insulin actually does.
- You eat food containing carbohydrates.
- Your digestive system breaks carbs down into glucose, which enters your bloodstream.
- Your pancreas releases insulin, a hormone that acts like a key.
- Insulin “unlocks” your cells so glucose can enter and be used for energy.
- Blood sugar levels drop back to a normal range.
Diabetes happens when this system breaks down — either because there’s no key (Type 1) or because the locks stop working properly (Type 2).
Type 1 vs. Type 2 Diabetes: Comparison Table
| Feature | Type 1 Diabetes | Type 2 Diabetes |
|---|---|---|
| Cause | Autoimmune attack on insulin-producing beta cells | Insulin resistance plus declining insulin production |
| Insulin production | Little to none | Normal or high at first, declines over time |
| Typical onset age | Often children, teens, or young adults (can occur at any age) | Usually adults over 45, but rising in younger people |
| Onset speed | Rapid — days to weeks | Gradual — months to years, often unnoticed |
| Body weight link | No strong link to weight | Strongly linked to excess weight, especially abdominal fat |
| Family history role | Moderate genetic link | Strong genetic and lifestyle link |
| Prevention possible? | Not currently preventable | Often preventable or delayable |
| Treatment | Lifelong insulin (injections or pump) required | Lifestyle changes, oral medications, sometimes insulin |
| Reversibility/remission | Not reversible | Remission possible with significant weight loss |
| Share of diabetes cases | About 5–8% | About 90–95% |
What Causes Type 1 Diabetes?
Type 1 diabetes is classified as an autoimmune disease. For reasons researchers don’t fully understand, the immune system identifies the insulin-producing beta cells in the pancreas as a threat and destroys them.
Once enough beta cells are gone, the body can no longer produce insulin on its own. Without insulin, glucose builds up in the bloodstream instead of fueling the body’s cells.
Known risk factors include:
- Family history of Type 1 diabetes (though most people diagnosed have no affected relatives)
- Certain genetic markers
- Environmental triggers, such as specific viral infections, that may set off the immune response
- Geography — Type 1 diabetes is more common in some countries than others, suggesting environmental factors play a role
Lifestyle, diet, and body weight do not cause Type 1 diabetes. This is one of the most persistent myths about the condition, and it’s worth repeating: nothing the person did or ate triggered it.
What Causes Type 2 Diabetes?
Type 2 diabetes develops through a different mechanism called insulin resistance. The pancreas still produces insulin, but muscle, liver, and fat cells stop responding to it efficiently.
Picture insulin as a key and your cells as locks. In Type 2 diabetes, the locks get “sticky.” The key still fits, but it takes more effort to open the door. At first, the pancreas compensates by producing extra insulin — a state called hyperinsulinemia. Over years, that extra effort wears the pancreas down, and insulin output starts to drop.
Key risk factors include:
- Excess body weight, particularly around the abdomen
- Physical inactivity
- Family history — risk rises to roughly 40% with one parent affected and around 70% with both parents affected
- Age over 45 (though diagnoses in younger adults and adolescents are increasing)
- Prediabetes
- History of gestational diabetes
- Certain ethnic backgrounds, including Black, Hispanic, Native American, and Asian American populations, which carry higher risk
Unlike Type 1, Type 2 diabetes has clear, modifiable risk factors. That’s why prevention and even remission are realistic goals for many people.
Symptoms: How They Show Up Differently
Both types share core symptoms because both involve high blood sugar. But how fast those symptoms appear — and how obvious they are — differs sharply.
Shared symptoms:
- Excessive thirst
- Frequent urination
- Fatigue
- Blurred vision
- Slow-healing cuts or sores
- Unexplained weight loss
Type 1 diabetes symptoms tend to appear suddenly, often over days or a few weeks. They can be severe enough to require emergency care, especially if diabetic ketoacidosis (DKA) develops — a dangerous buildup of blood acids that happens when the body has no insulin at all.
Type 2 diabetes symptoms often develop so gradually that people don’t notice them for months or years. Many people are diagnosed only after a routine blood test, sometimes after complications have already begun. This is why Type 2 diabetes is frequently called a “silent” condition in its early stages.
How Each Type Is Diagnosed
Doctors use similar blood tests for both types, but additional testing helps tell them apart.
Standard diagnostic tests:
- A1C test – measures average blood sugar over 2–3 months; 6.5% or higher indicates diabetes
- Fasting plasma glucose test – measures blood sugar after an overnight fast
- Oral glucose tolerance test – measures blood sugar before and after drinking a sugary solution
- Random plasma glucose test – used when symptoms are severe and immediate testing is needed
To distinguish Type 1 from Type 2, doctors may also order:
- Autoantibody tests – detect immune markers specific to Type 1 diabetes
- C-peptide test – measures how much insulin the pancreas is still producing
- Ketone testing – checks for ketoacidosis, more common in Type 1
A correct diagnosis matters because treatment approaches diverge significantly from this point forward.
Treatment Differences
Type 1 Diabetes Treatment
Because the body produces no insulin, people with Type 1 diabetes need insulin therapy for life. There’s no alternative — diet and exercise alone cannot replace insulin the pancreas no longer makes.
Common treatment tools include:
- Multiple daily insulin injections or an insulin pump
- Continuous glucose monitors (CGMs) to track blood sugar in real time
- Carbohydrate counting to match insulin doses to food intake
- Regular blood sugar checks throughout the day
Type 2 Diabetes Treatment
Type 2 diabetes treatment usually follows a step-up approach, starting with the least invasive options.
- Lifestyle changes – weight management, regular physical activity, and a balanced diet are often the first line of treatment
- Oral medications – such as metformin, which improves insulin sensitivity
- Injectable non-insulin medications – including GLP-1 receptor agonists, which support blood sugar control and often weight loss
- Insulin therapy – added if other treatments no longer maintain healthy blood sugar levels
Some people with Type 2 diabetes who lose a significant amount of weight, particularly soon after diagnosis, achieve remission, meaning their blood sugar returns to normal without medication. Remission is not considered a cure, since the condition can return, but it is a meaningful and achievable goal for many.
Can You Prevent Type 1 or Type 2 Diabetes?
This is one of the most searched questions on this topic, and the answer differs sharply between the two types.
Type 1 diabetes cannot currently be prevented. Because it’s driven by an unpredictable autoimmune response, there’s no known lifestyle change, diet, or supplement that stops it from developing.
Type 2 diabetes can often be prevented or delayed. Large-scale studies have shown that modest weight loss, regular physical activity, and dietary changes can cut the risk of developing Type 2 diabetes substantially in people with prediabetes. Even when prevention isn’t fully possible, these same changes can delay onset by years.
By the Numbers: How Common Is Each Type?
- Type 2 diabetes accounts for roughly 90–95% of all diabetes cases worldwide.
- Type 1 diabetes makes up about 5–8% of cases.
- In the United States, an estimated 2.1 million people have diagnosed Type 1 diabetes, including 1.8 million adults and roughly 314,000 children and adolescents.
- More than 40 million Americans — about 12% of the population — live with diabetes overall.
- An estimated 1.5 million new cases of diabetes are diagnosed in the U.S. every year.
- Over 115 million American adults are living with prediabetes, a major risk factor for Type 2 diabetes.
These numbers explain why Type 2 diabetes dominates public health messaging — but they shouldn’t overshadow the very real and distinct challenges of living with Type 1.
Common Myths, Corrected
Myth: Type 1 is “juvenile diabetes,” and only kids get it. False. Type 1 diabetes can develop at any age, including in adults in their 30s, 40s, and beyond. “Juvenile diabetes” is an outdated term doctors no longer use.
Myth: Type 2 diabetes only affects people who are overweight. Not entirely true. While excess weight is a major risk factor, genetics, age, and ethnicity also play significant roles. People at a healthy weight can develop Type 2 diabetes.
Myth: Eating too much sugar causes diabetes. Misleading. Sugar alone doesn’t directly cause either type. Type 1 is autoimmune. Type 2 is linked to overall diet quality, weight, and activity level — not sugar in isolation.
Myth: You can tell which type someone has just by looking at them. False, and harmful. Body size, age, and appearance are not reliable indicators of diabetes type.
When to See a Doctor
Talk to a healthcare provider promptly if you notice:
- Sudden, intense thirst and urination
- Unexplained weight loss
- Persistent fatigue that doesn’t improve with rest
- Fruity-smelling breath, nausea, or confusion (possible signs of DKA — seek emergency care)
- A family history of diabetes combined with any early symptoms
Early diagnosis, for either type, significantly reduces the risk of long-term complications like nerve damage, kidney disease, and vision loss.
Frequently Asked Questions
What is the main difference between Type 1 and Type 2 diabetes? Type 1 diabetes is an autoimmune condition where the body makes little or no insulin. Type 2 diabetes occurs when the body still makes insulin but can’t use it effectively, a state called insulin resistance.
Which type of diabetes is worse, Type 1 or Type 2? Neither type is universally “worse.” Type 1 requires lifelong insulin from day one and can be harder to manage day-to-day. Type 2 develops more slowly but carries serious long-term complication risks if left untreated. Both require consistent management.
Can Type 2 diabetes turn into Type 1? No. They have different underlying causes, and one does not convert into the other. However, some adults are initially misdiagnosed with Type 2 when they actually have a slow-developing autoimmune form called LADA (latent autoimmune diabetes in adults).
Is Type 1 diabetes genetic? Genetics play a role, but most people diagnosed with Type 1 diabetes have no family history of it. Environmental triggers likely interact with genetic susceptibility.
Can Type 2 diabetes be reversed? Type 2 diabetes can go into remission, especially with significant weight loss soon after diagnosis. Remission means blood sugar returns to a normal range without medication, though ongoing monitoring is still recommended since the condition can return.
Do both types require insulin? Type 1 always requires insulin. Type 2 sometimes requires insulin, usually after other treatments are no longer enough to control blood sugar, but many people manage it without insulin for years or indefinitely.
At what age does each type usually appear? Type 1 most often appears in children, teens, and young adults, but it can develop at any age. Type 2 traditionally appears after age 45, though rates among children and younger adults are rising due to lifestyle and obesity trends.
Can someone have both Type 1 and Type 2 diabetes? It’s uncommon but possible to have features of both, sometimes referred to as “double diabetes.” This typically occurs when a person with Type 1 diabetes also develops insulin resistance, often related to weight gain.
Key Takeaways
- Type 1 diabetes is autoimmune; the body produces little to no insulin and requires lifelong insulin therapy.
- Type 2 diabetes is driven by insulin resistance and often progresses gradually, with treatment ranging from lifestyle changes to medication and, eventually, insulin.
- Type 2 diabetes is far more common, making up roughly 90–95% of cases, while Type 1 accounts for about 5–8%.
- Type 2 diabetes can often be prevented or delayed; Type 1 cannot currently be prevented.
- Symptoms overlap, but Type 1 tends to appear suddenly, while Type 2 develops slowly and quietly.
- An accurate diagnosis is essential, since treatment plans differ significantly between the two types.
If you’re experiencing symptoms or have risk factors for either type, don’t wait for things to get worse. Schedule a blood sugar screening with your doctor — early detection is the single most effective step you can take to protect your long-term health.

